Dallas
214-456-2240
Fax: 214-456-8881
Plano
469-497-2501
Fax: 469-497-2507
Request an Appointment with codes: Plastics and Craniofacial Surgery
214-456-2240
Fax: 214-456-8881
469-497-2501
Fax: 469-497-2507
Request an Appointment with codes: Plastics and Craniofacial Surgery
Sagittal craniosynostosis (scaphocephaly) is the most common form of isolated craniosynostosis. Patients with this pattern of suture closure make up about half of all craniosynostosis cases. All skull bone growth occurs perpendicular or growing away from the suture. The sagittal suture runs lengthwise along the top of the skull from front to back, therefore the growth at this suture gives the skull its width.
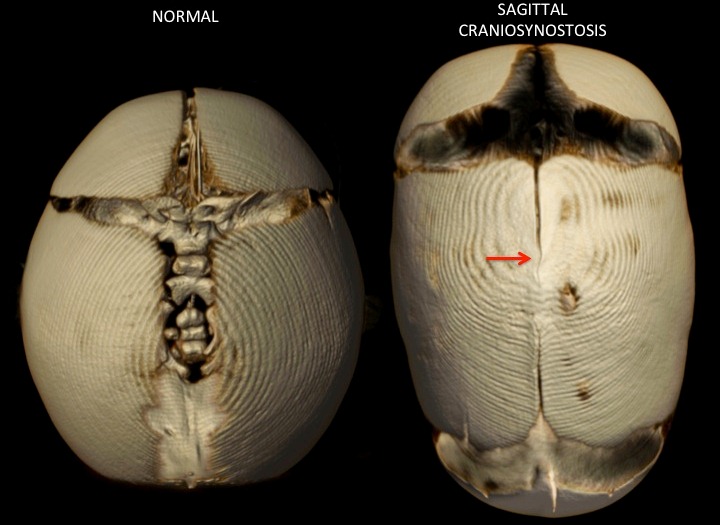
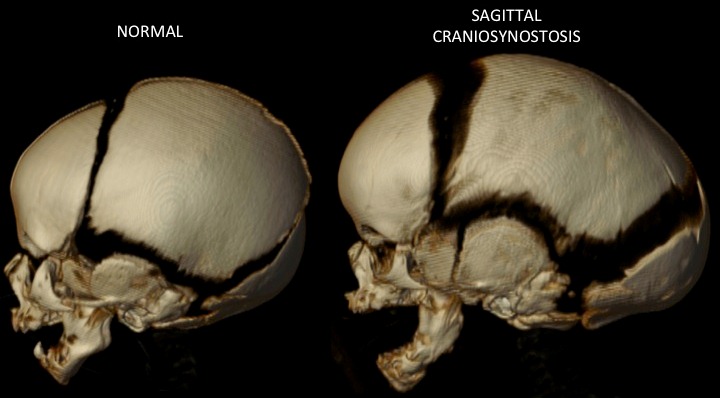
When the sagittal suture is closed the skull can’t widen, so the remaining open sutures must create more bone to make room for the growing brain. The orientation of the remaining open sutures – the coronal, lambdoid and metopic sutures – can only create bone perpendicular to their axis.
Sagittal Craniosynostosis Before and After photos
The lack of bone growth at the sagittal suture and extra bone growth at the remaining open sutures makes the head longer and narrower than usual. In some children, there is more fullness (bossing) of the forehead. In others, the back of the head may be more significantly affected with a longer, narrow and coned shape. In some patients, the changes in shape may be even distributed from front to back. Boys tend to have this type of craniosynostosis more than girls with a ratio of 4 boys to each girl with this defect.
There is no one operation that works well for all patients. In general, the treatment strategy depends on the age of the patients at the time of diagnosis.
An extended strip craniectomy with postoperative helmet therapy is the treatment of choice. This approach provides good correction in head shape, with a shorter operation and hospitalization and lower risk for blood transfusion when compared to open cranial vault procedures.
After surgery, we place the baby in a custom-fit molding helmet. This helmet fits up against the forehead and back of the head and does not apply pressure. Instead, it resists growth in these directions. The skull then grows to a more normal shape because the brain takes the path of least resistance and widens pushing the bones as it expands.
Patients diagnosed after four months of age are too old for extended strip craniectomy surgery. This is because after 4 months of age the skull bones quickly become too thick and stiff for sufficient reshaping with the helmet. As surgeons, we must customize our surgical plan to each child’s skull deformity. Most often in these cases, we will use an open cranial vault remodeling for these patients.
Often this is limited to reconstructing the back two-thirds of the skull in one operation. The full forehead seen in most of these patients tends to correct on its own once the back is reconstructed. Occasionally, in severe cases, separate operations are needed to correct the front and the back of the skull. These surgeries are done in stages with a period of 3-6 months between procedures to allow for recovery between the procedures.
There are many approaches to open cranial vault remodeling in sagittal synostosis. In general, the skull bones are removed in the areas of abnormal restricted and compensatory growth and repositioned to over correct the head shape and increase the space in the skull. In general, for sagittal suture craniosynostosis the surgeries are aimed at restoring normal dimensions in the width, height and length of the skull. Rarely, surgeons use cranial vault distraction.